The mainstream narrative for pattern baldness is that testosterone gets converted into dihydrotestosterone (DHT) by an enzyme called 5α-reductase. DHT then binds to the androgen receptors in hair follicle cells which causes the hair follicle to miniaturise over the course of multiple hair cycles.
Eventually, the miniaturised hair follicle produces extremely thin, wispy and barely perceptible strands of hair. There are mountains of scientific evidence supporting this thesis.
However, focusing solely on DHT as the cause of baldness leaves a lot of unanswered questions.
- If DHT is the only cause of hair thinning, why is it that hair loss incidence increases with old age while DHT levels drop in old age?
- Why is it that balding scalps have lower subcutaneous blood flow?
- DHT miniaturises hair follicles. But why is DHT higher in balding scalps than in non-balding scalps?
- Why does hair recession tend to occur in a pattern (temples and crown first)?
- Why does pattern hair loss not appear to occur on the back and sides of the head?
- Why does DHT cause hair loss on the scalp, but is associated with hair growth in the body?
This study by researcher Paul Taylor mentions that the “skull often appears larger and more bulbous in shape for those who experience severe AGA (androgenic alopecia) relative to those who do not.” Could this help explain some of the questions above?
Some people on internet forums claim first hand that their head shapes are exacerbating their hair loss.
On the pother hand, others claim that this theory is complete bogus.
So, does head size bare any influence on wether or not we lose our hair? Is head size the primary cause of baldness, simply a secondary complicit accomplice to DHT or does it play no role at all?
In this article, we answer these questions.
Skull shape and hair loss. Is there a link?
DHT is a primary driver of male pattern hair loss. What a lot of people don’t know, is that DHT also has an anabolic effect on bone formation.
Androgen receptor sites, 5α-reductase and DHT all exist within certain types of bone cells. DHT can stimulate the proliferation of osteoblast cells and the formation of new bone.
An article from Duke university mentions that “using CT scans of 100 men and women, the researchers discovered that the bones in the human skull continue to grow as people age. The forehead moves forward while the cheek bones move backward. As the bones move, the overlying muscle and skin also move, subtly changing the shape of the face”.
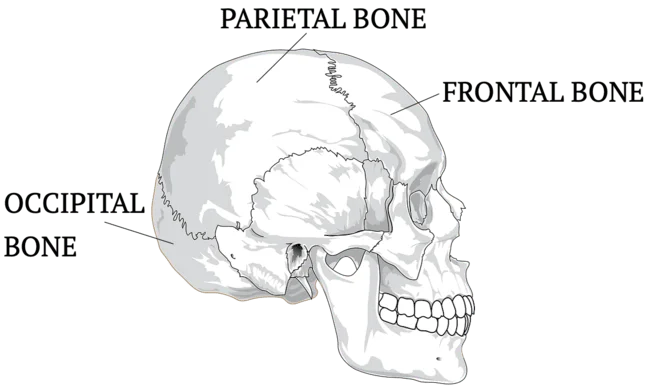
For reference, the main skull bones can be seen below.
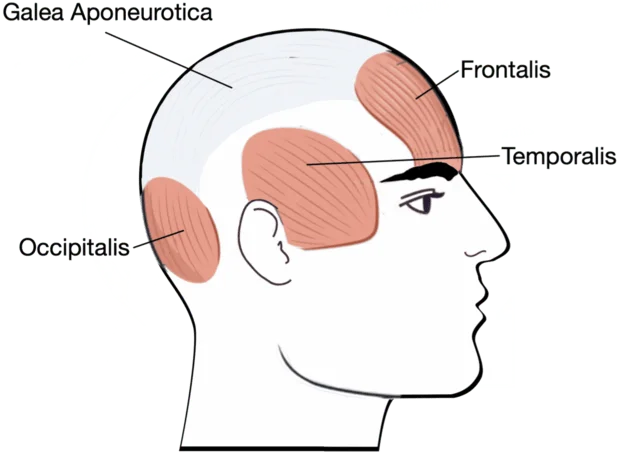
Overlying the exact regions of the skull on which pattern hair loss occurs, we have the galea aponeurotica. This is a layer of dense dense fibrous connective tissue that extends over the scalp. The muscles that surround the scalp perimeter anchor the Galea in place.
Multiple studies have shown that balding regions of the scalp have lower oxygenation (due to vascular insufficiency) than non-balding regions of the scalp. Another study revealed that compared to non-balding scalps, balding scalps on average, have 2.6 times lower subcutaneous blood flow rate.
Healthy blood supply to the hair follicle is essential for the maintenance and growth of strong and thick hair strands. After all, blood is the carrier vehicle for oxygen and nutrients which feed cell proliferation across the body.
Putting it all together
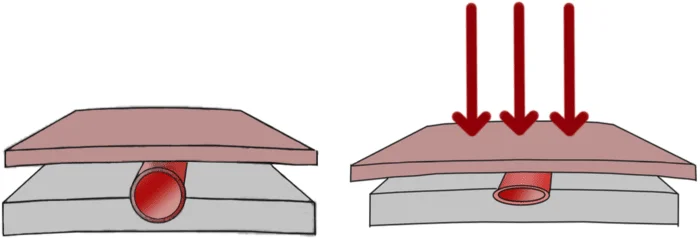
The study by Paul Taylor asserts that the expansion of the frontal and parietal bones can stretch overlying tissue thereby increasing scalp tension.
This tension, according to the study, can constrict the blood vessels on the top scalp, lowering oxygen and nutrient supply to the hair follicle, leading to hair follicle miniaturisation.
Do we have any other evidence to support this theory?
Dr. Brian Freund conducted an experiment where he injected botox (a muscle relaxant) into he scalp perimeter muscles of the study patients. By relaxing the scalp perimeter muscles, the scalp become ‘looser’ and less tense. This improved blood flow and oxygen concentration in the top of the scalp and increased hair counts by 18% after 48 weeks.
Furthermore, a finite element analysis study sought to find out wether mechanical stress is involved in androgenic alopecia. They measured the stress on a model of the galea aponeurotica. They found that the stress distribution on the scalp closely resembles the pattern in which hair loss usually progresses.
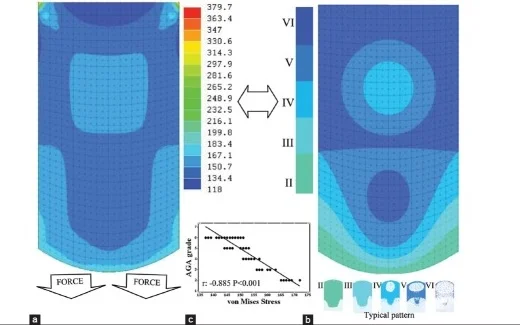
The study concluded that “mechanical stress determines AGA (androgenic alopecia) patterning and a stretch-induced and androgen-mediated mechanotransduction in dermal papilla cells could be the primary mechanism in AGA pathogenesis”.
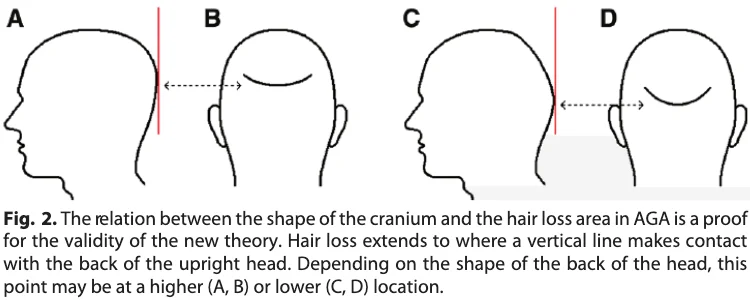
Dr. Ustuner, a plastic surgeon from Turkey, agrees and points out that individual hair loss patterns are affected by differences in the shape of the head, reflecting variations in scalp pressure.
Here is a snippet from Dr. Ustuner journal.
Female skulls and hair loss
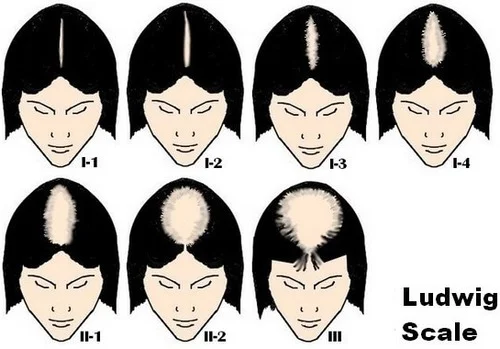
Women can experience female pattern hair loss (FPHL). In women, pattern hair loss tends to follow the Ludwig chart.
FPHL can (like with men) be driven by androgens. This is the case for women with hirsutism or sometimes, women with PCOS. However, this study shows that “FPHL may develop even in the absence of androgens”.
Women on average, have smaller skulls than men partially due to the lower levels of androgen hormones which can drive bone growth. Furthermore, women have higher oestrogen (compared to men) which according to Dr. Ustuner “protects the cushioning tissues until after meno-pause in the female”.
We know that post-menopausal women see a decrease in oestrogen levels. This decline in oestrogen has been associated with pattern baldness.
Dr. Ustuner proposes that the fat tissue immediately surrounding the hair follicle helps cushion the hair follicles against the scalp pressure. While estrogen helps maintain the integrity off this subcutaneous fat layer, “subcutaneous fat tissue starts to decrease instantaneously at an early age in the male due to increase in testosterone levels.”
After menopause, estrogen level drops may no longer protect this fat layer in the scalp, making the hair follicles more exposed to the effects of scalp pressure.
Paul Taylor confirms that “low (post-menopausal) oestrogen levels have been associated with AGA”. His journal suggests that “This may reflect that, relative to pre-menopausal oestrogen levels, testosterone levels will be higher, and so the bone resorption, remodelling and skull expansion processes will all increase for those women with the genetic predisposition towards AGA.”
All in all, it seems as though hormonal changes in post-menopausal women can sometimes lead to changes in skull structure and/or scalp tissue that can in turn manifest as hair loss.
PCOS and skull shape
Female hair loss sufferers with polycystic ovarian syndrome (PCOS) tend to see more of a ‘male pattern baldness’ hair loss progression compared to female hair loss sufferers without PCOS.
This is likely because one of the hallmarks of PCOS is an increase in male hormones.
A study showed that long-term PCOS can lead to an increase in bone mineral density in the skull. This is because the hormonal imbalance associated with PCOS encourages further skull bone growth in early puberty and throughout adulthood.
Craniofacial development and hair loss. Is there a link?
Over the last few centuries, we (human beings) have experienced some dramatic changes in our lifestyles and upbringing despite having largely the same genetic makeup as our ancestors from thousands of years ago. Some cultural and lifestyle shifts include:
- An increase in bottle-feeding babies over breast-feeding. This influences the swallowing pattern and oral muscle action 1,2,3,4.
- The use of pacifiers/dummies that mainly affect tongue posture 5,6,7,8.
- A trend towards soft, high-calorie foods that lower chewing effort and muscles action 9,10,11.
- An increase in allergies and nasal congestion that has lead to more mouth breathing. This influences both tongue posture and muscles action 12,13,14,15,16.
The effect tongue posture has on craniofacial development can be a whole 500 page book in and of itself.
The high level summary is that bones remodel under the presence of continuous forces. Different habits and lifestyles encourage different resting tongue positions (i.e resting at the top vs. at the bottom of the mouth) which result in a different force distribution and therefore changes the shape of the face and skull 17, 18, 19, 20.
Our ancestors have generally had straight teeth as a result of their lifestyles.
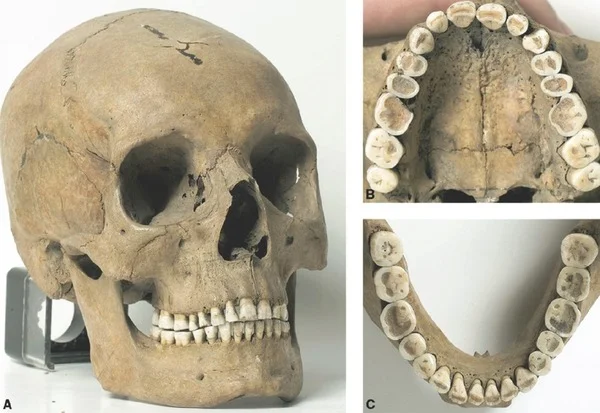
It turns out that dental irregularities such as malocclusion are a modern problem. Weston Price documented the stark contrast in teeth alignment between indigenous tribes with traditional diets (hard foods requiring lots of chewing) and lifestyle against tribes who has adopted westernised processed (soft) diets. Just one generation apart, the contrast is startling.
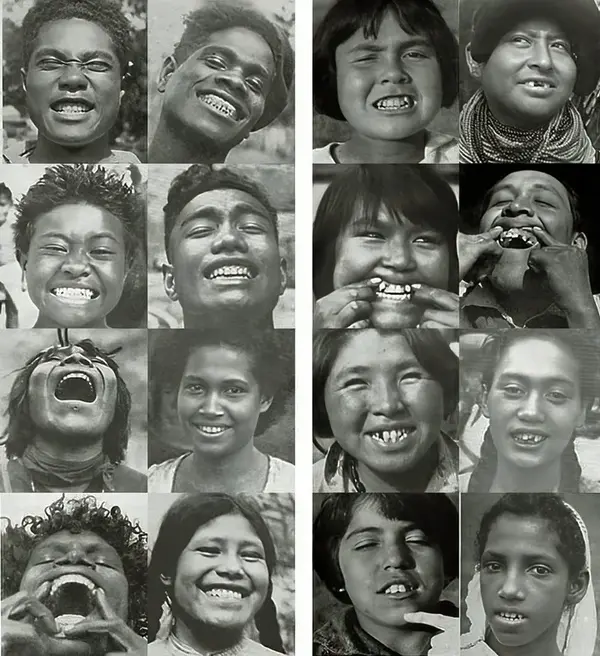
Here’s a quote from ‘The Jaw Epidemic: Recognition, Origins, Cures, and Prevention’: ”Despite claims that the cause of this jaw epidemic is somehow genetic, the speed with which human jaws have changed, especially in the last few centuries, is much too fast to be evolutionary.”
Teeth mis-alignment and hair loss
What is the link between skull shape, teeth alignment and hair loss?
This study mentions that “through a series of observational case studies, it is evident that there is a relationship between malocclusion and hair loss”. The study suggests that the architecture of the skull associated with malocclusion obstructs blood flow from the superior temporal artery to the top off the scalp.
We know that dental mis-alignment has become increasingly commonplace. Interestingly, hair loss incidence may also be not the rise.
Leonora Doclis, a senior trichiologost mentioned that “the average age that a man starts to experience hair loss is declining and the number of those affected are growing”. The growing incidence of hair loss is likely due to a number of different factors. Could skull changes be partly responsible for the growing incidence of androgenic alopecia?
I can think of many people with perfectly aligned teeth and great facial structures who have experienced severe pattern baldness. For example, Jeremy Meeks. On the flip side, I can also think of people with teeth mis-alignment who have retained full heads of hair.
Whilst not the centre piece, perhaps skull architecture is a piece of the puzzle that is pattern baldness.
Final thoughts
I maintain that DHT plays a central role in pattern baldness. But perhaps skull size can influence scalp perimeter muscle contraction and help explain some questions the DHT model cannot explain by itself.
Scrutiny of this skull-shape hair loss model will invariably lead to more questions. But, there certainly seems to be compelling evidence for head shape and size as being a factor that can influence certain facets of hair loss (namely, hair loss pattern and possibly rate of thinning).

Pingback: Dave
Awesome blog.
What about the tongue? Has anybody thought of that? The tongue struggles when the palate is too short or not smooth. The tongue requires support of the palate, a counteractive force. If it struggle it can lead to cranial strains. The tongue also struggle if pharyngeal airway is shrunk because the mouth is shrunk and tongue and mandible pushed back, so the body has to force forward head posture to open airways. That also put strain on the head.
I think it’s especially the posterior part of the tongue that when struggling due to palatal bone too short or bent, it can’t get up and have correct suction posture and it falls down and this leads to cranial strains. The digastric muscle and so on have to take over the tongue’s job by forcing it up of the airways.
I guess it could be compressed TMJs too.
If not smooth or long enough palate, the tongue struggles if there is no proper hard and smooth place, and right height in the palate to settle it.
With the orthodontic profession shrinking faces and jaws en masse with premolar extractions and braces, the anterior-posterior of the face/jaws shrink. Having the palate, the lower maxilla, shrunk and bent is a huge problem for so many things of the skull, jaws and the body, especially for the teeth, tongue, airways, and TMJs.